Key Takeaways
America's most invasive export isn't McDonald's, it's our definition of madness

The real cultural contamination is psychiatric. Watters argues that while we worry about exporting fast food and pop music, our most homogenizing influence is teaching the world to experience mental illness the American way. Through the DSM (psychiatry's diagnostic bible, now a global standard), Western-trained clinicians, drug company marketing, and trauma counselors who parachute into disaster zones, we have flattened a once-astonishing diversity of human suffering.
Madness was never uniform. Indonesian men experienced amok (brooding that erupts into murderous rage), Southeast Asian men suffered koro (the terror that genitals are retracting into the body), and Victorian women collapsed with hysterical leg paralysis. These forms appear and vanish with their cultures. Watters calls the researchers documenting them botanists racing ahead of bulldozers.
What's striking is how Watters inverts the usual globalization complaint. Critics fret about cultural imperialism in consumer goods, yet the psyche itself rarely enters that conversation. The claim resonates with medical anthropologist Arthur Kleinman's concept of illness as culturally constructed, and with Ian Hacking's idea of transient mental illnesses that flourish in particular ecological niches of belief. A fair challenge: biological psychiatry would counter that brain disorders have universal neural substrates regardless of cultural dress. Watters does not deny biology, but insists the expression and experience of suffering is inseparable from local meaning. That nuance is easy to lose in his more polemical framing.
Naming a disorder publicly can summon the very epidemic you fear
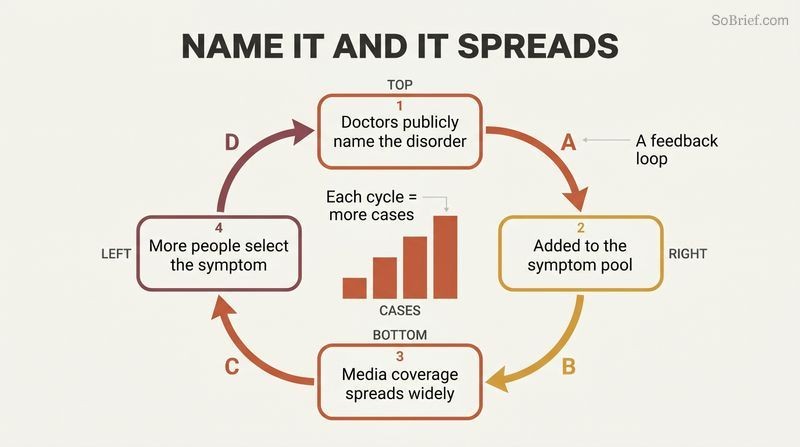
The symptom pool theory. Medical historian Edward Shorter argues that people in distress unconsciously select symptoms from a culturally available menu, a symptom pool, choosing whatever signals legitimate suffering in their time. When doctors publicly name and debate a disorder, they add it to that pool, and a feedback loop follows: media coverage, more patients, more attention, more cases.
Anorexia proves the pattern twice. Self-starvation was rare until Charles Laségue formally named hysterical anorexia in 1873, after which Western cases climbed steeply. It faded by the 1940s, then surged again after singer Karen Carpenter died of it in 1983. In Hong Kong, a 14-year-old's 1994 death on a busy street triggered identical coverage, and cases that had been two or three a year became that many per week.
This is the book's most unsettling mechanism: awareness campaigns may function as transmission vectors. The bulimia data are eerily supportive. British cases tracked Princess Diana's public struggle almost perfectly, rising with each revelation and declining after her death, yet the original researchers never even considered imitation as an explanation. The idea echoes sociologist David Phillips's work on copycat suicides (the Werther effect) and modern concerns about social-contagion in self-harm communities online. The uncomfortable implication for public health: destigmatization and education, however well-intentioned, are never neutral acts. They reshape the menu of expressible distress, sometimes enlarging the very problem they target.
Hong Kong's anorexics didn't fear fat until the West taught them to
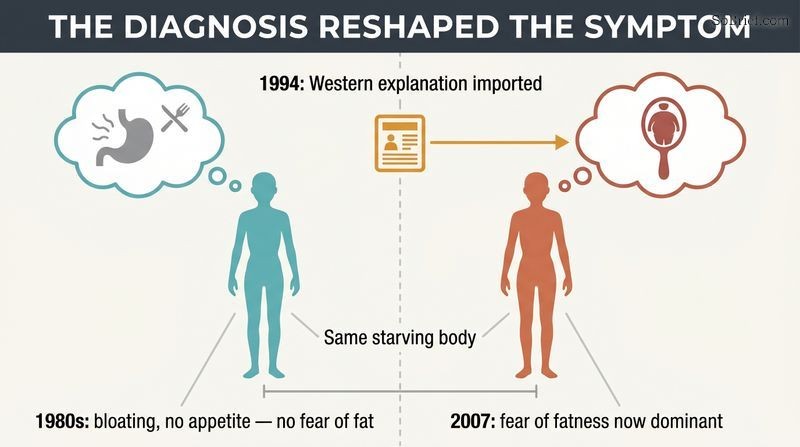
Atypical anorexia revealed a hidden truth. Psychiatrist Sing Lee documented Chinese anorexics in the 1980s who starved themselves but, unlike Western patients, expressed no fear of fatness and no distorted body image. They explained their refusal through bodily sensations: bloating, stomach blockages, no appetite. One patient, Jiao, weighed 48 pounds yet drew herself accurately and only wanted to reach a normal weight. These patients matched nineteenth-century European cases that predated the modern fat-phobia template.
Then the symptoms changed. After Charlene Hsu's 1994 death imported the Western explanation wholesale, fat phobia became the dominant stated reason. By 2007 nearly all of Lee's patients reported it. The diagnosis did not just describe the disease, it reshaped the actual subjective experience.
Lee's natural experiment is anthropologically precious because it caught a disorder mid-transformation. It complicates the lazy assumption that Barbie dolls and thin models cause eating disorders. Acculturation studies repeatedly failed to find that link, and some found immigrants who held to traditional values had MORE disordered eating. The deeper lesson concerns somatization: Chinese culture, lacking the sharp Cartesian mind-body split, channels psychological distress into physical idioms. A Western teen says she feels anxious; a Hong Kong teen of that era felt her stomach was blocked. Both are real. The pathology adapts to whatever vocabulary of suffering a culture makes legible.
Trauma counselors flooding disaster zones often help themselves more than survivors

The largest psychological intervention in history backfired. After the 2004 tsunami killed over a quarter-million people, hundreds of Western trauma counselors descended on Sri Lanka assuming PTSD reactions are universal. They competed for refugee camps, relied on tourist-trade drivers as therapy translators, and one organization counseled 1,724 people in a few days. Many had no grasp of local language, religion, or burial rituals, and some treated this ignorance as an asset, claiming to be non-political and non-denominational.
The certainty was misplaced. Studies through the 1990s showed early debriefing was ineffective or harmful. Car-accident victims who were debriefed were MORE anxious and fearful three years later. Counselors sometimes implanted memories in suggestible survivors, asking leading questions that manufactured the symptoms they expected to find.
Watters frames the rush as a gold rush of credentialed compassion, and the evidence is damning. Critical incident stress debriefing, once mandatory after Western disasters, is now discouraged by major bodies precisely because trials showed it could impede natural recovery. The deeper critique draws on Vanessa Pupavac's argument that the West's trauma evangelism reflects our own post-Cold-War insecurity projected outward. A steelman for the counselors: showing up signals solidarity, and material aid often rode alongside the therapy. But Watters's point stands. When the helper's framework assumes universal fragility, it can pathologize resilience and silence local healing systems that actually worked.
Sri Lankans locate trauma's damage in broken relationships, not broken brains
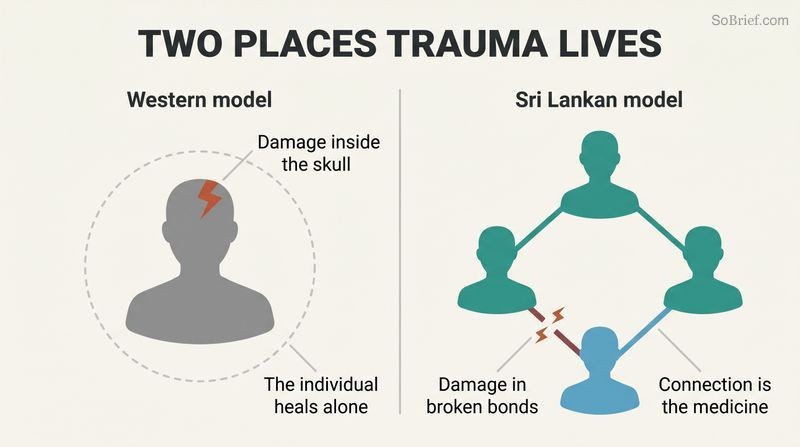
Suffering can live outside the skull. Psychologist Gaithri Fernando, instead of imposing PTSD checklists, asked Sri Lankans open-ended stories about who recovered and who didn't. She found two key differences from the American model. First, Sri Lankans experienced trauma physically, complaining of joint, muscle, and chest pain. Second, and more profound, they located the damage in the social world: the inability to fulfill one's role in the family or kinship group was the primary symptom, not a consequence of inner psychological injury.
This flips the treatment logic. In the West, you take sick leave to heal the individual mind, then return to social duties. For a Sri Lankan, withdrawing from social roles to do solo counseling with a stranger could worsen the problem, because connection itself is the medicine.
Fernando's interview method, building local idioms of distress from the ground up rather than translating a foreign questionnaire, is methodologically superior to the parachute surveys that merely confirmed what they assumed. Her finding maps onto the broader individualist-versus-collectivist literature: in sociocentric cultures the self is fundamentally relational, so injury to the web is injury to the person. A poignant illustration: a boy who lost his father felt comforted not by promises of safety but by his mother's vow that the family would die together. Western therapy would read that as morbid. In context it is the deepest possible reassurance, a guarantee of unbroken belonging.
In Sri Lankan villages, NOT talking about violence kept the killing contained

Silence was a social technology. Anthropologist Alex Argenti-Pillen studied a village scarred by civil war and a youth uprising, where neighbors had informed on, tortured, and killed one another yet still lived side by side. Villagers used an elaborate dialect of cautious words to reference horror without invoking it: torture became a child's mischief, the brutal war became the confusion of people who hurry too much. Speaking graphically of violence could spread the gaze of the wild, an affliction that turned victims violent.
Western counseling threatened the truce. Trauma workers insisted survivors must retell and master their experiences directly. The villagers who eagerly adopted this were the fearless women, already socially dangerous for their sharp tongues. Counseling legitimized them, potentially removing the brakes on cycles of revenge.
This is the book's most provocative reversal: the PTSD orthodoxy treats avoidance as pathology to be overcome, yet here circumspect speech was a deliberate, collective peacekeeping mechanism. The insight reframes what therapists call denial as something closer to wisdom. It connects to transitional-justice debates, where truth-telling commissions are usually assumed healing, but anthropologists note that in tight communities, strategic forgetting can prevent reprisal. The risk Argenti-Pillen identifies, that imported trauma discourse could reignite violence, is the gravest charge in the book. It suggests cultural humility is not mere politeness but a safety requirement, since interventions can destabilize equilibria invisible to outsiders.
Schizophrenics recover better in poor countries than rich ones
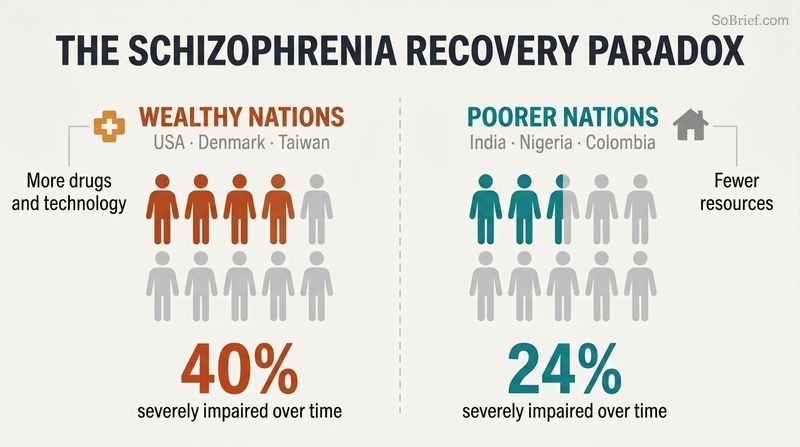
The most provocative finding in cross-cultural psychiatry. Two large World Health Organization studies tracked over a thousand patients across a dozen sites for decades. Those diagnosed in India, Nigeria, and Colombia had longer remissions and better social functioning than patients in the United States, Denmark, or Taiwan. Roughly 40 percent of patients in industrialized nations became severely impaired over time, versus 24 percent in poorer countries. The places with the best drugs, technology, and research had the most disabled patients.
Emotional climate may explain it. Research on expressed emotion shows schizophrenics relapse far more often in families high in criticism, hostility, and emotional overinvolvement. Relapse rates ran around 50 percent in high-emotion households versus 21 percent in low-emotion ones, a pattern holding across cultures.
The irony is brutal and well-replicated: resources do not equal outcomes. The expressed-emotion research offers a mechanism, and Jill Hooley's work adds a twist. Highly critical relatives tend to have an internal locus of control, believing people master their own fate, a trait Americans prize as can-do spirit. Applied to a sick relative, that optimism becomes corrosive pressure. Anglo-American families scored highest in expressed emotion at 67 percent. The finding should humble wealthy nations, though caveats apply: diagnostic criteria, dropout rates, and what counts as recovery vary across sites. Still, the core pattern has survived reanalysis, and it indicts the assumption that biomedicine alone heals.
Calling mental illness a brain disease increases stigma, not compassion
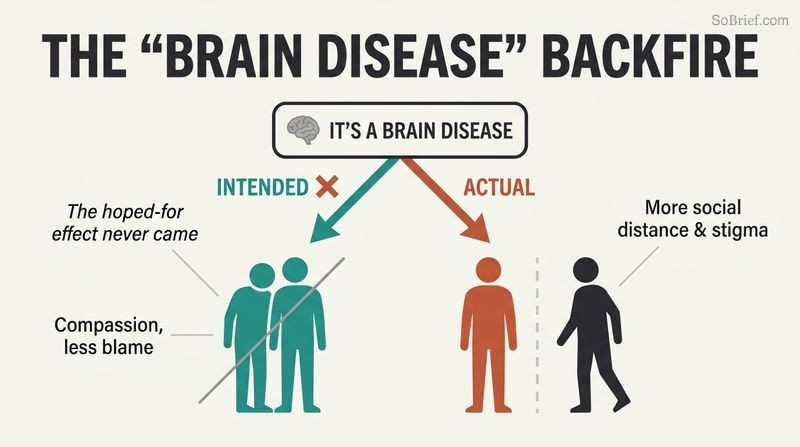
The well-intentioned strategy backfired. Advocates pushed the biomedical narrative, mental illness as a disease like any other, believing it would absolve sufferers of blame. Yet as the world adopted chemical-imbalance and genetic explanations over fifty years, perceptions of dangerousness rose, not fell. Studies in Turkey, Germany, Russia, and Mongolia found that people who endorsed biological causes wanted MORE social distance from the mentally ill.
Why brokenness feels permanent. A genetic or biochemical story implies the person is fundamentally and irreversibly abnormal, almost a different species. In Sheila Mehta's experiment, subjects told a partner had a biological disease delivered harsher electric shocks than those told the problem stemmed from childhood events. In Zanzibar, by contrast, spirit-possession beliefs kept the ill person inside the social group.
This finding upends a generation of anti-stigma messaging built on the disease model. The logic is subtle: explanations that remove blame can simultaneously remove agency and hope. If your serotonin is simply broken, you are less culpable but also less redeemable, and more frighteningly other. The Zanzibari spirit narrative, though scientifically false, performed better socially because spirits come and go, allowing remission to be read as the person returning. Patient memoirs cited by Watters capture the cost: reducing love, grief, and ecstasy to just chemistry strips meaning from selfhood. The practical takeaway is that how we frame causation shapes how we treat people, sometimes perversely.
Drug companies don't just sell cures, they market the diseases first
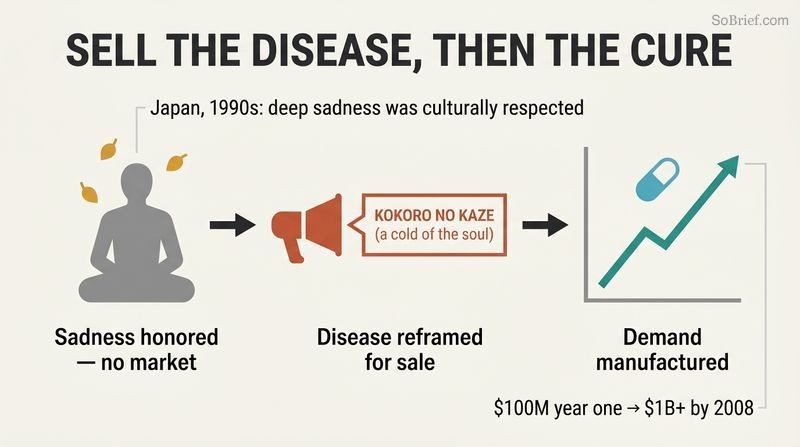
Mega-marketing engineers demand. Anthropologist Kalman Applbaum showed how pharmaceutical firms entering Japan aimed to alter the total environment in which a drug is used, reshaping consciousness itself. In the 1990s, Japan had no mass market for antidepressants because deep sadness was culturally honored, not pathologized. The word for clinical depression, utsubyo, denoted a rare, psychotic-level condition.
GlaxoSmithKline changed the culture. Before launching Paxil, the company flew cross-cultural scholars to luxury conferences to learn how Japanese beliefs about sadness had formed. Their winning slogan recast depression as kokoro no kaze, a cold of the soul: stigma-free, common, and easily medicated. Combined with publicity around overwork suicides like that of young ad-man Oshima Ichiro, sales hit 100 million dollars the first year and over a billion by 2008.
Applbaum's boardroom anthropology is rare and valuable, showing marketing not as persuasion about a product but as construction of the need itself. The Japanese case is especially clean because the prior cultural resistance was so explicit: melancholy was a mark of depth and sensitivity, tied to Buddhist views of suffering and to the prized melancholic personality type. What's chilling is the executives' sincerity. They believed they were spreading first-world medicine and healing the world. The serotonin-imbalance story they sold has no scientific consensus behind it. This connects to critiques of disease-mongering, where ordinary distress gets rebranded as treatable pathology to expand a market.
The chemical-imbalance theory of depression was a marketing line, not science
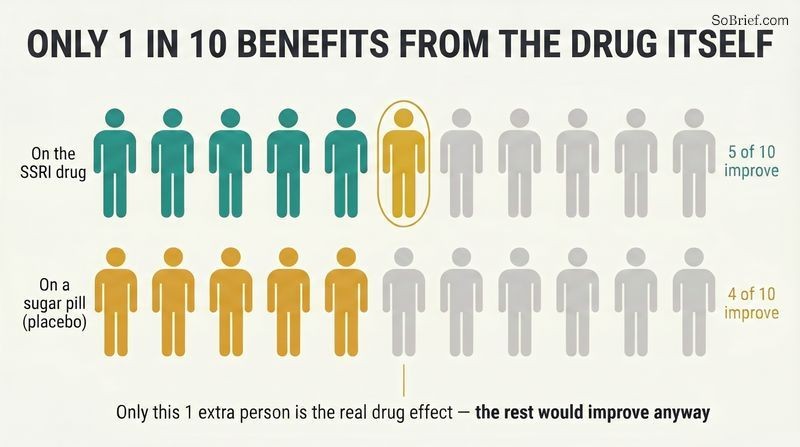
A story without evidence. The claim that depression stems from low serotonin, repeated in ads worldwide, lacks scientific consensus. George Ashcroft proposed it in the 1950s, then abandoned it by 1970 when better measurements found no serotonin deficit in depressed patients. SSRIs broadly alter brain chemistry; they do not restore a documented natural balance. Psychiatry's own clinical textbook states the depletion hypothesis was never confirmed.
The data pipeline is compromised. Psychiatrist David Healy estimates drug companies ghostwrote over half the studies in top journals by the mid-1990s. Of 38 positive antidepressant trials, 37 were published; of 36 negative trials, only 3 appeared. When all data are pooled, roughly five in ten patients improve on an SSRI versus four in ten on placebo, meaning only one in ten shows a drug-specific benefit.
The publication-bias figures are the quiet scandal here, since invisible negative trials inflate apparent efficacy across all of medicine, not just psychiatry. Erick Turner's later FDA analyses confirmed the lopsided publishing Watters describes. The serotonin myth's durability is itself a case study in how a convenient narrative outlives its evidence because it serves multiple parties: companies get a sales hook, doctors get a simple script, patients get a blame-free explanation. None of this proves antidepressants are useless; they clearly help some people, particularly in severe cases. The honest position is humility about mechanism and effect size, which the marketing actively obscured, especially when crossing into cultures already wary of psychotropics.
Times of social upheaval make cultures defenseless against imported mental illnesses
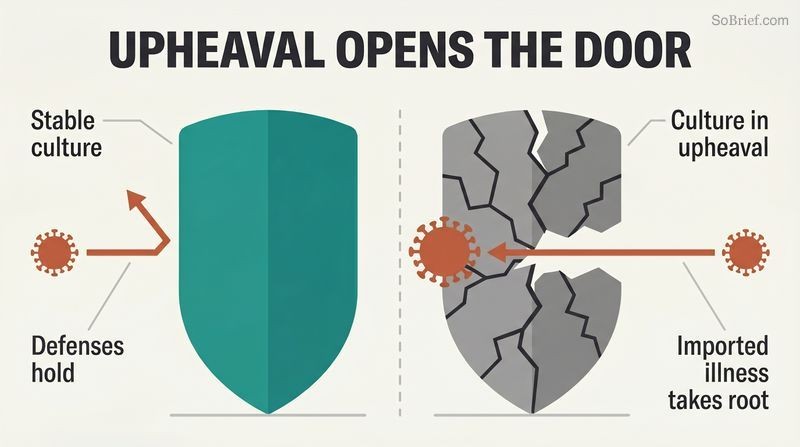
Distress seeks the available template. Watters notes each epidemic took root during disorientation. Anorexia spread in Hong Kong during the anxious years between the 1989 Tiananmen crackdown and the 1997 handover to China. PTSD colonized populations reeling from war and disaster. The American depression took hold during Japan's long recession. When status, security, and the future feel threatened from everywhere at once, populations reach for whatever explanation the moment offers.
The next opening is now. As Watters wrote during the 2008 global financial crisis, experts were already announcing recession-driven mental-health epidemics and 301 new psychiatric drugs in development. A candidate diagnosis, post-traumatic embitterment disorder, was first identified among East Germans destabilized by the Berlin Wall's fall, perfectly suited to the insecurity of rapid global change.
This is the book's macro-thesis: cultural immune systems weaken under stress, and Western categories rush into the vacuum. The pattern rhymes with historical episodes of mass psychogenic phenomena that cluster in periods of social strain, from medieval dancing manias to Victorian hysteria. Watters's closing provocation deserves weight: offering Western psychiatric frameworks to soothe globalization's anxieties may worsen the root problem, because those very frameworks erode the local beliefs and relational selves that once gave suffering meaning. The hyperindividualist, hyperintrospective American mind, he argues, is a poor model to universalize, especially given how much contentment it has actually delivered. A sobering note to end on, deliberately unresolved.
Analysis
Crazy Like Us is a work of narrative medical anthropology disguised as reportage, and its structure (four deep case studies bookended by argument) is both its strength and its limitation. The strength is vividness: Sing Lee mimicking anorexia to understand it, the tsunami gold rush of counselors, Zanzibar's spirit-tolerant households, GlaxoSmithKline's geisha-served conferences. The limitation is that four anecdotal case studies cannot fully bear the weight of a six-billion-person thesis, and Watters occasionally lets polemic outrun evidence.
Intellectually, the book sits at the convergence of three traditions: Ian Hacking's transient mental illnesses and ecological niches, Arthur Kleinman's category fallacy (applying a culture-bound construct as if universal), and the social-constructionist critique of psychiatric nosology. Watters's distinctive contribution is journalistic synthesis plus a focus on transmission mechanisms: the symptom pool, the feedback loop, mega-marketing, and the parachute intervention. He shows how a category travels, not just that it does.
The deepest and most defensible claim is that meaning is constitutive of mental illness, not decorative. The Sri Lankan locating trauma in social roles and the Chinese anorexic feeling a blocked stomach are not mistranslations of a universal disease; they are different diseases as lived. This is philosophically serious and empirically supported by the expressed emotion and WHO schizophrenia data.
The book's blind spot is that it can read as romanticizing the premodern, though Watters explicitly disclaims this, insisting other cultures have it different, not necessarily right. A second tension: he relies on Western science (publication-bias studies, debriefing trials) to debunk Western psychiatry, which is methodologically fine but worth noting. Written before replication-crisis awareness peaked, its critique of pharmaceutical data has aged remarkably well. The enduring takeaway is epistemic humility: exporting our psyche is neither neutral nor obviously benevolent.
Review Summary
Crazy Like Us examines how Western mental health concepts are being exported globally, often causing harm. Watters explores anorexia in Hong Kong, PTSD in Sri Lanka, schizophrenia in Zanzibar, and depression in Japan, demonstrating how mental illness manifests differently across cultures. Reviewers praise the book's compelling case studies and critique of pharmaceutical companies and Western psychological imperialism. Some criticize the journalistic approach as lacking depth or being unprofessional. Most find it thought-provoking and essential reading for understanding cultural influences on mental health, though concerns exist about cherry-picked data and oversimplification.
People Also Read
Glossary
Symptom pool
Culture's menu of expressible distressEdward Shorter's term for the limited set of culturally legitimate symptoms that people in psychological distress unconsciously draw upon to express suffering. When doctors publicly name and validate a new disorder, they add it to the pool, making it more likely people will manifest those symptoms. Symptoms drift in and out of the pool over time as their power to communicate distress rises and fades.
Expressed emotion
Family emotional climate around patientsA measure of how much criticism, hostility, and emotional overinvolvement family members direct at a mentally ill relative. Pioneered by George Brown in 1950s England, high expressed emotion strongly predicts schizophrenia relapse: roughly 50 percent versus 21 percent in low-emotion households. The pattern holds across cultures, and Anglo-American families score highest, partly explaining better schizophrenia outcomes in poorer nations.
Mega-marketing
Reshaping a culture to sellKalman Applbaum's term for pharmaceutical strategy that goes beyond selling a product to altering the entire cultural environment in which it might be used. Rather than just advertising a drug, companies reshape public beliefs about a disease, who is at risk, and what symptoms mean, effectively manufacturing demand by redefining normal experience as treatable pathology.
Atypical anorexia
Self-starvation without fat phobiaSing Lee's term for the form of anorexia he documented in 1980s Hong Kong, in which patients starved themselves but had no fear of fatness and no distorted body image, instead attributing food refusal to bodily sensations like bloating or loss of appetite. It resembled pre-twentieth-century European cases and largely disappeared once the Western fat-phobia template was imported.
Kokoro no kaze
Depression as cold of soulJapanese marketing phrase meaning a cold of the soul, used by GlaxoSmithKline to reframe depression for the Japanese public. It carried three messages at once: depression is mild and stigma-free, treating it is as routine as taking cold medicine, and it is as common as catching a cold. The slogan helped transform Japanese attitudes and drove Paxil sales past a billion dollars.
Gaze of the wild
Sri Lankan affliction from violenceIn the cosmology of a Sinhalese Buddhist village studied by Alex Argenti-Pillen, the experience of being looked at by a wild spirit during moments of terror, which can leave a person violent, immobilized, or somatically ill. Crucially, speaking graphically about violence was believed capable of spreading the affliction, which is why villagers used euphemistic cautious words to contain cycles of revenge.
Typus melancholicus
Sadness-prone idealized personalityThe melancholic personality type introduced by Hubert Tellenbach, marked by orderliness, high personal standards, and deep concern for others' welfare. Influential in Japanese psychiatry, it associated proneness to overwhelming sadness with prized cultural traits, making melancholy something to aspire to rather than fear, and partly explaining Japan's initial resistance to viewing depression as an illness.
FAQ
What is Crazy Like Us: The Globalization of the American Psyche by Ethan Watters about?
- Global spread of American psychiatry: The book examines how American psychiatric concepts and diagnoses, such as anorexia, PTSD, schizophrenia, and depression, are being exported worldwide, reshaping local understandings of mental health.
- Cultural shaping of mental illness: Watters argues that mental illnesses are not universal but are deeply influenced by cultural beliefs, social contexts, and historical moments.
- Case studies as evidence: Through detailed stories from Hong Kong, Sri Lanka, Zanzibar, and Japan, the book illustrates the complex interplay between Western psychiatric models and local traditions.
- Consequences of globalization: The narrative highlights both the intended and unintended effects of imposing Western mental health frameworks globally, including increased stigma and loss of indigenous healing practices.
Why should I read Crazy Like Us by Ethan Watters?
- Challenges Western assumptions: The book encourages readers to question the universality of Western psychiatric diagnoses and treatments, revealing the cultural biases embedded in mental health care.
- Broadens cultural perspective: It provides a nuanced understanding of how mental illness is experienced and managed differently across cultures, moving beyond the Western biomedical model.
- Exposes pharmaceutical influence: Watters uncovers how drug companies shape cultural narratives about mental illness to expand markets for medications.
- Cautionary insights: Readers gain awareness of the risks and unintended consequences of globalizing Western mental health concepts without cultural sensitivity.
What are the key takeaways from Crazy Like Us by Ethan Watters?
- Mental illnesses are culturally shaped: Disorders like anorexia, PTSD, and schizophrenia are not fixed entities but are deeply influenced by local beliefs and social contexts.
- Globalization homogenizes mental illness: The export of American psychiatric categories and treatments often erases local understandings and can cause harm.
- Cultural sensitivity is crucial: Effective mental health care requires understanding and respecting local beliefs and practices rather than imposing Western models.
- Unintended consequences: Well-meaning interventions can inadvertently reinforce or spread mental illnesses by shaping cultural symptom pools and disrupting indigenous healing traditions.
How does Ethan Watters in Crazy Like Us explain the cultural shaping of mental illness?
- Culture as symptom shaper: Mental illnesses manifest differently depending on cultural beliefs, social roles, and historical context, meaning the same disorder can look very different across societies.
- Symptom pools and templates: The book introduces the concept of a “symptom pool,” where certain symptoms become culturally available ways to express distress, and new illness categories can spread rapidly.
- Cultural feedback loops: Interactions between medical professionals, media, and patients reinforce certain illness expressions, influencing the rise or decline of specific mental illnesses within a culture.
- Idioms of distress: Watters highlights that people use culturally specific ways to express psychological suffering, which may not align with Western diagnostic categories.
What are the main case studies in Crazy Like Us and what do they illustrate?
- Anorexia in Hong Kong: The transformation of anorexia’s symptoms and meaning after Western psychiatric concepts entered public consciousness, leading to a rise in Western-style cases.
- PTSD in Sri Lanka: The imposition of Western trauma models after the 2004 tsunami, which often clashed with local beliefs and healing practices.
- Schizophrenia in Zanzibar: How spirit possession and Islamic teachings shape family responses, often resulting in better outcomes than in Western contexts.
- Depression in Japan: The marketing of Western depression concepts and antidepressants, which altered traditional Japanese views of sadness and mental health.
How does Crazy Like Us by Ethan Watters critique the globalization of PTSD after the 2004 tsunami in Sri Lanka?
- Western assumptions imposed: Mental health professionals assumed PTSD was a universal response to trauma and applied Western diagnostic and treatment models without sufficient cultural understanding.
- Cultural disconnect: Sri Lankan beliefs emphasize social relationships and somatic symptoms, with local healing traditions playing a crucial role in recovery.
- Potential harm of interventions: The influx of Western trauma counselors sometimes disrupted local social dynamics and healing practices, destabilizing communities.
- Undermining indigenous coping: Imposing Western models can unintentionally undermine local resilience and coping mechanisms.
What does Crazy Like Us by Ethan Watters reveal about schizophrenia in Zanzibar and the role of expressed emotion?
- Better outcomes in developing countries: Research shows people with schizophrenia in Zanzibar often have better long-term outcomes than those in industrialized nations.
- Cultural beliefs and family dynamics: Spirit possession and religious teachings shape understanding and management, with families showing low expressed emotion (criticism, hostility).
- Emotional environment matters: Calm, tolerant family environments in Zanzibar may contribute to improved prognosis, contrasting with high-stress Western households.
- Expressed emotion defined: High expressed emotion in Western families is linked to beliefs in personal control and accountability, which can increase stress for patients.
How does Crazy Like Us by Ethan Watters address the role of pharmaceutical companies in the globalization of mental illness?
- Profit motives: Drug companies have financial incentives to promote universal disease categories, expanding markets for their medications worldwide.
- Marketing diseases: Pharmaceutical companies market not just drugs but the very diseases they treat, shaping public and professional perceptions of mental illness.
- Influence on treatment paradigms: This commercial influence reinforces the biomedical model and accelerates the spread of American mental health concepts globally.
- Ethical concerns: The book exposes ghostwriting, data suppression, and manipulation of scientific studies to promote medications like SSRIs.
What does Crazy Like Us by Ethan Watters say about the marketing and cultural transformation of depression in Japan?
- Mega-marketing campaign: Pharmaceutical companies launched campaigns to redefine Japanese cultural understandings of depression, creating a market for SSRIs like Paxil.
- Traditional views of sadness: Japan historically valued melancholy as a natural or even virtuous state, not a medical illness.
- "Cold of the soul" metaphor: Marketers reframed depression as kokoro no kaze, a common and treatable illness, to reduce stigma and encourage medication use.
- Scientific and ethical controversies: The book details how companies manipulated data and downplayed side effects to promote antidepressants.
What is the significance of the DSM and American psychiatric categories in Crazy Like Us by Ethan Watters?
- DSM as global standard: The American Psychiatric Association’s DSM has become the worldwide reference for diagnosing mental illnesses, exporting American concepts globally.
- Homogenization of mental illness: DSM categories, developed in a specific cultural context, are being applied universally, often ignoring local variations and meanings.
- Impact on diagnosis and treatment: Universal application can obscure culturally specific symptoms, leading to misdiagnosis and ineffective or harmful treatments.
- Loss of local understanding: The spread of DSM categories can erase indigenous idioms of distress and healing traditions.
What are the key concepts introduced in Crazy Like Us by Ethan Watters about mental illness and culture?
- Symptom pool: A cultural repertoire of symptoms available for expressing psychological distress, which changes over time and place.
- Expressed emotion: A family environment characterized by criticism, hostility, and emotional overinvolvement, linked to worse outcomes in schizophrenia.
- Cultural feedback loop: The dynamic interaction between medical professionals, media, and patients that shapes the prevalence and expression of mental illnesses.
- Idioms of distress: Culturally specific ways people express and experience psychological suffering, which may not align with Western diagnostic categories.
What are the broader implications and lessons for global mental health from Crazy Like Us by Ethan Watters?
- Cultural humility needed: Mental health interventions must respect and integrate local beliefs and practices rather than impose Western models uncritically.
- Risks of globalization: Exporting Western psychiatric categories can increase stigma, disrupt local healing, and sometimes worsen suffering.
- Pharmaceutical influence: The globalization of mental illness is intertwined with corporate marketing strategies that shape cultural understandings for profit.
- Call for rethinking: Watters advocates for more culturally sensitive, socially grounded approaches to mental health care worldwide.
Download PDF
Download EPUB
.epub digital book format is ideal for reading ebooks on phones, tablets, and e-readers.

































