Key Takeaways
A Texas hospital for the poor beats America's best on cost and outcomes
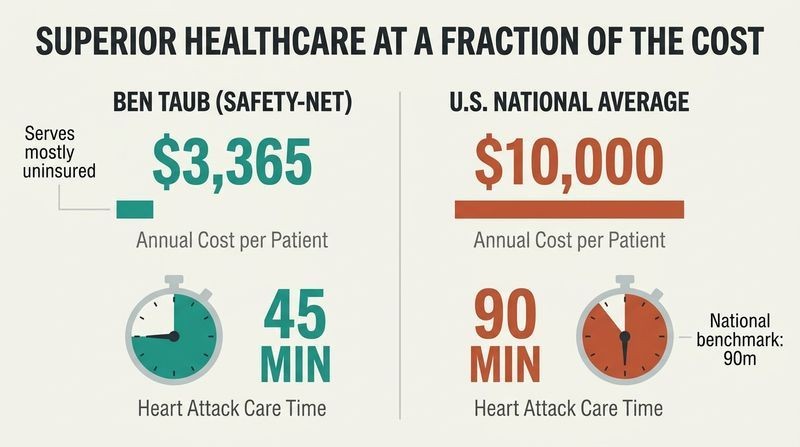
The counterintuitive core claim. Ben Taub, Houston's largest safety-net hospital, serves mostly uninsured patients (63% completely uninsured, only 7% privately insured) yet spent roughly $3,365 per patient in 2015 against a national average near $10,000. It matched the efficiency of French and German systems while delivering elite results.
Proof in the numbers. In 2015 Ben Taub was rated the best hospital in the country for treating heart attacks. With just four cath labs and three interventional cardiologists, it unblocked clogged coronary arteries in an average of 45 minutes, half the typical 90-minute national benchmark. Nuila's metaphor: a heart attack is like a kinked garden hose starving a lawn, and Ben Taub restored flow fastest, producing the "greenest lawns."
The claim punctures a deep American assumption that price signals quality. Health economists have long documented this disconnect: the Dartmouth Atlas showed higher-spending regions often deliver worse outcomes. What's striking is Ben Taub's mechanism, a fixed public budget that removes the fee-for-service incentive to do more. One caveat worth holding: safety-net hospitals also benefit from case-mix and teaching-hospital volume effects that sharpen skills, so efficiency and excellence may be partly downstream of scale rather than purely of funding structure. Still, the counterexample matters because it proves affordable and excellent are not mutually exclusive in American medicine.
Having insurance is not the same as being able to afford care
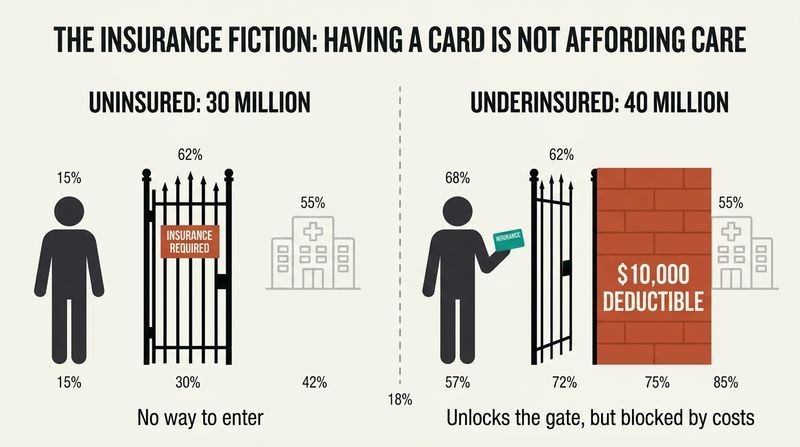
The insurance fiction. Stephen Hart, a successful burger-chain manager earning $75,000, chose the cheapest plan at $88 per paycheck. When a lump in his neck turned out to be tonsil cancer, he prepaid $639 just to enter the ER, then was told by a specialist: "However, you don't have insurance." He meant sufficient insurance. A social worker sent him to Ben Taub.
The scale of the gap. About 30 million Americans are uninsured, but another 40 million are underinsured, meaning deductibles and out-of-pocket costs (sometimes $10,000 before benefits begin) make care unaffordable even with a card. That totals roughly 20% of the population effectively locked out. A 2019 study found 66% of US bankruptcies, over 530,000 families a year, stem from medical bills.
Nuila targets a blind spot in political debate that treats the insured/uninsured binary as the whole story. The underinsured are politically invisible because they appear covered. This connects to research on high-deductible health plans, which reduce both wasteful and necessary care, since patients cannot distinguish the two at the point of rationing. Stephen's story also reveals a behavioral trap: rational-seeming frugality (skipping premiums when healthy) becomes catastrophic precisely because illness is unpredictable. The deeper point is that insurance was originally sold as peace of mind, yet modern plans deliver anxiety and surprise bills, inverting the product's founding promise.
Fee-for-service turned doctors into businesspeople who profit from sickness
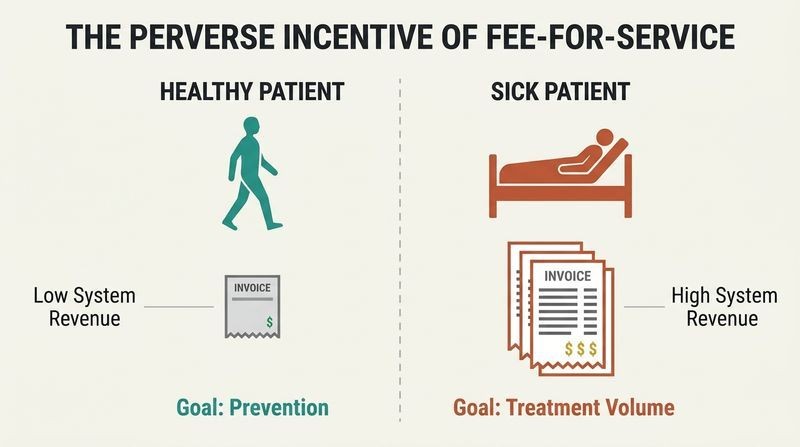
How medicine became a business. Historically American doctors insisted on setting their own fees, billing patients separately from hospitals. The 1934 AMA principles enshrined "no third party between patient and physician" and direct patient billing. This became fee-for-service: doctors bill for each service rendered, not outcomes. If a surgeon left a rag inside a patient, he could bill twice, once to remove it.
The perverse incentive. Nixon named the "illogical incentive": sickness pays doctors and insurers more than keeping people healthy. Costs grew at three times inflation through the 1970s. By the 1980s, two of ten doctors earned incomes in the top 1%, making 80% more than European peers. As one insurer CEO put it, the goal was healthcare as reliable a product as a Big Mac.
Nuila, whose own father ran a private OB-GYN practice, writes this as family history, which lends it credibility beyond ideology. The analysis echoes Paul Starr's Pulitzer-winning work on how American doctors "escaped becoming victims of capitalism and became small capitalists instead." What deserves scrutiny: fee-for-service is not uniquely American, and capitated or salaried systems carry their own distortions, such as under-treatment and gatekeeping that frustrated patients in 1990s HMOs. The honest framing is that every payment model rations somehow. Fee-for-service simply rations toward excess and away from the poor, which is the specific failure mode Nuila diagnoses.
Insurance was invented to sell peace of mind, not to enrich middlemen
The schoolteacher origin. In 1929 Baylor administrator Justin Ford Kimball, facing a failing hospital, offered Dallas teachers 21 days of hospitalization for 50 cents a month. Over 75% enrolled. This was the birth of group coverage and the ancestor of Blue Cross. The insight: covering one person is expensive, but larger pools make coverage affordable.
How it mutated. World War II wage freezes (1942 Stabilization Act) let employers offer health benefits as a loophole to attract workers, birthing employer-sponsored insurance. A 1954 tax change made benefits tax-deductible. By 1955, 70% of Americans had insurance through work. Insurance companies entered as brokers to manage "moral hazard," the tendency to overconsume when someone else pays, like piling food at an all-you-can-eat buffet.
The history reframes today's system as accident rather than design, which is both liberating and damning. If employer-based insurance emerged from a wartime wage-control loophole, there is nothing sacred or inevitable about it. Economists still debate moral hazard's magnitude: the RAND Health Insurance Experiment and the Oregon Medicaid study both found more insurance increases utilization, though whether that care is wasteful or beneficial remains contested. Kimball's story carries a quiet irony Nuila exploits well: the original product genuinely served patients and hospitals simultaneously, before insurers inserted themselves as profit-taking intermediaries and flipped the incentive structure toward denial and delay.
Ask "sick or not sick," never "insured or not insured"
The decisive question. When Roxana, an undocumented Salvadoran woman with dry gangrene from a botched cancer surgery, arrived at Ben Taub's ER, the doctors admitted her based on one question: sick or not sick? At a nonprofit hospital, Nuila argues, a doctor could have glanced at her signs of infection, judged her technically "stable," prescribed antibiotics she couldn't afford, and discharged her. That doctor "wouldn't have been wrong," but wouldn't have been right.
Why the framing matters. Roxana was uninsured and undocumented, ineligible for ACA insurance, Medicaid, or Medicare. A home hospice nurse had been sent to help her "auto-amputate" her dead limbs over years, essentially sending her home to die. Ben Taub admitted her, treated the infection, and eventually amputated her legs, restoring a path to prosthetics and independence.
This is the moral engine of the book, and it operationalizes an abstract value into a concrete clinical decision rule. The power lies in showing that the same patient triggers opposite behaviors depending on the institution's financial structure, not the doctor's character. This aligns with research on how organizational incentives shape individual ethics more than personal virtue does. A useful tension: "sick or not sick" still requires rationing downstream, since Ben Taub cannot offer transplants. So the rule governs admission, not unlimited treatment. The genius is separating the triage gate from cost, which is precisely where American medicine most corrupts clinical judgment.
Textbook medicine assumes a patient who was already treated
The Pocket Medicine blind spot. As a student, Nuila met a woman in her forties with dementia, incontinence, and darting eyes. He suspected early Alzheimer's or rare disorders. His mentor Dr. Graham corrected him: untreated diabetes had caused thousands of tiny strokes. The condition was common and manageable, but she had lacked access. Nuila's medical handbook listed no diagnosis called "a life without health insurance."
Access rivals genetics. A 2017 review found insurance reduces premature death by up to 6%, comparable to aspirin's effect on heart attacks. The Oregon Medicaid lottery showed coverage dramatically improved diabetes diagnosis and management. Diabetes costs roughly $4,800 per year even for the insured, nearly 10% of an average salary, so the uninsured face a mountain they cannot climb.
Nuila's reframing, that lack of insurance belongs on the differential diagnosis alongside biological causes, is genuinely original clinical thinking. It resonates with the "social determinants of health" literature, which estimates medical care accounts for only 10-20% of health outcomes while social and behavioral factors drive the rest. The teaching case is powerful because the woman's dementia was irreversible by the time she arrived, illustrating how delayed access converts cheap, preventable problems into expensive, permanent ones. The critique implicit here targets medical education itself: training doctors on idealized bodies that already received care leaves them blind to the epidemiology of poverty.
Beware algorithmania: forcing patients onto decision trees to look decisive
A coined diagnosis for doctors. Nuila defines algorithmania as the compulsive use of clinical decision trees even when a patient's complexity should keep them off. It makes the doctor, not the patient, the protagonist: satisfy the flowchart and you feel you've satisfied the patient. A diabetic mentioning vague chest pressure gets funneled into the chest-pain algorithm, shipped by ambulance, and worked up for a heart attack she may never have had, while her real complaint goes unasked.
The personal cost. Nuila's own grandmother complained she couldn't swallow. He ran the dysphagia algorithm, ordered a barium swallow that came back normal, and missed her esophageal cancer for six months. He blames himself not for her death but for her suffering, and for choosing a flowchart over a real conversation about her prognosis.
Algorithmania is a sharp addition to the vocabulary of medical error, complementing Atul Gawande's more optimistic case for checklists. The tension between the two is instructive: checklists prevent lapses in routine procedures, while algorithms fail in ambiguous diagnosis where human judgment and patient narrative matter most. Cognitive scientists would call this the difference between well-structured and ill-structured problems. Nuila's Haiti anecdote, where a neurosurgeon ruled out a brain bleed with a sternal rub and a Glasgow Coma Scale score instead of a scan, shows the corrective: algorithms as tools that complement judgment, never replace it, and never chase illusory 100% certainty.
Twenty cents of every US healthcare dollar is pure waste
Waste, not scarcity, is the enemy. Christian Garza, a young man with mysterious knee pains, bounced through ERs, a rheumatologist who wouldn't see him until visit two, a Mexican stem cell clinic, and denied insurance claims before finally being diagnosed with rare Fabry disease. His care failed not from lack of resources but from their disorganized excess. Former Medicare chief Donald Berwick identified six categories of waste; Christian suffered at least five, including failed care coordination, overtreatment, and administrative complexity.
The staggering figure. Berwick estimated 20% of all healthcare spending, roughly $200 billion a year, is waste. That same sum could cover every uninsured American. Nuila's point: America doesn't need to spend more on healthcare, it needs to spend better, because the money to cover everyone already exists inside the system.
This reframe is politically potent because it sidesteps the exhausting "how do we pay for it" objection. If the funding already exists as waste, universal coverage becomes a reallocation problem, not a new-spending problem. Berwick's taxonomy remains influential, though critics note "waste" is easier to name than to extract, since one actor's waste is another's revenue, which is exactly why it persists. Christian's odyssey also illustrates a subtler cost economists call the patient's time and suffering as an externality never counted on any ledger. Five years of a young life lost to pain appears in no budget, yet represents the truest cost of fragmentation.
$179 too much income cost a 36-year-old his life
A margin that killed. Geronimo, brought to the US at nine, worked despite epilepsy at gas stations and restaurants, paying into Social Security. When hepatitis C and diabetes destroyed his liver, he needed a transplant, which required Medicaid. He qualified, then lost it, because his $912 monthly disability check exceeded Texas's limit by $179. In any Medicaid-expansion state, his income would have qualified easily.
The bureaucratic rescue that came too late. Nuila's team appealed to Geronimo's congressman and the state Medicaid director. Astonishingly, coverage was approved. But by then his failing liver had caused a brain bleed. He was removed from the transplant list and died one month to the day after arriving. Near the end, treated with sudden attention, he told his mother: "Everyone treats me like I'm rich."
Geronimo's case is the book's most devastating indictment because the lethal factor was arithmetic, not medicine. It exposes the "coverage cliff," a design flaw where earning slightly more triggers total loss of benefits, punishing exactly the work ethic policy claims to reward. Behavioral economists call these notches, and they distort incentives cruelly at eligibility boundaries. The geographic lottery compounds the injustice: identical illness, identical income, opposite outcomes depending on state lines. That an individual congressional appeal could override the rule reveals the system's arbitrariness, since salvation depended on having a doctor willing to make phone calls rather than on any consistent principle of desert.
We accept broken healthcare because we can't imagine anything better
Disaster syndrome, diagnosed. Nuila borrows the term from novelist Jan de Hartog, who during a 1953 Dutch flood found an exhausted doctor almost resentful of rescue: he had adapted to catastrophe and accepted it as permanent. The syndrome sets in when normal outrage at intolerable conditions vanishes, replaced by the urge to circumvent rather than correct.
How it manifests. Every time we read an article about healthcare's brokenness, shake our heads, and conclude nothing can change, we display disaster syndrome. Doctors show it through burnout: over half of American physicians cite bureaucracy as the top cause, and nearly half plan to cut hours or leave. Nuila's mentor and friend Dave, who embodied everything right about Ben Taub, died by suicide during the COVID surge, a shattering reminder that even the best system's people can break.
Naming resignation as a diagnosable condition is a rhetorical masterstroke, because it turns passivity into something actively pathological rather than merely realistic. The burnout reframe deserves emphasis: physicians increasingly argue the term blames victims for a broken system, preferring "moral injury," the wound of being forced to act against patients' interests. This borrows from combat psychology and shifts responsibility from individual resilience to institutional design. The connection to learned helplessness in psychology is direct: when people believe action is futile, they stop trying even when change becomes possible. Dave's death grounds the abstraction in unbearable specificity, refusing to let systemic failure remain a statistic.
The world's first hospital, in 550 AD Persia, charged no one
A single-tier ideal. Jundi-Shapur, meaning "Beautiful Garden," was a Persian teaching hospital where Greek, Jewish, Zoroastrian, and Indian doctors trained the next generation and treated any person, any race, any class, without payment. Rumors of it drew the sick across half a continent. It embodied science applied to illness without interference from money or authority.
America's fractured alternative. The US, by contrast, built tiers. Nuila proposes not necessarily Medicare for All (he doubts Americans would surrender the privacy and speed private insurance buys) but a two-tier system: a national standard of care for everyone regardless of citizenship, with the option to purchase more. The key is that choosing basic versus premium shouldn't mean the difference between life and death, as it did for Geronimo over $179.
Invoking a 1,500-year-old institution is more than ornament; it denaturalizes the tiered American system by proving universal, science-based care predates modern politics. Nuila's policy realism is notable: rather than dogmatically demanding single-payer, he concedes that privacy and speed have genuine value people will pay for, which most European systems accommodate through supplemental private insurance atop a universal floor. This pragmatic two-tier vision resembles Germany, France, and Australia more than Canada or Britain. The honest weakness he acknowledges is defining the floor: would it include liver transplants? Where the standard sits determines whether the second tier is a convenience or, as now, a lifeline.
Hope and dignity heal even when a cure is impossible
Faith as a building block. Nuila's daily faith comes not from religion but from the diverse staff who choose to work at a hospital for the poor when better-paying jobs beckon. Roxana, an undocumented amputee with metastatic cancer, converted to Islam years earlier and drew strength from prayer through every catastrophe. Denied prostheses by the safety net because her cancer was terminal, she got them through a Christian charity organized by strangers moved by her story.
The final image. Nuila last saw Roxana at her rehab "graduation," driving a donated peacock-blue power wheelchair she called her Mercedes, having learned to feed, toilet, and transport herself. American medicine says without a cure there is no hope. Ben Taub taught him these are separate: there can be cures without hope and hope without cures, but the miracles are human ones.
Ending on hope decoupled from cure resists the sentimentality the topic invites, because Nuila roots it in specifics: a wheelchair, a charity, a woman's independence, not vague uplift. The insight parallels the palliative care movement and Atul Gawande's argument that medicine's fixation on cure often fails the dying by neglecting what makes life meaningful. Roxana's dignity emerges precisely because Ben Taub's non-profit structure let clinicians attend to her personhood rather than her payer status. The subtle challenge to readers: hope here is not passive optimism but the product of a community deciding that a poor, undocumented, dying woman still deserved to feel, in Geronimo's words, treated like she was rich.
Analysis
The People's Hospital is a hybrid of memoir, medical ethnography, policy argument, and history, structured around five patients (Stephen, Roxana, Ebonie, Christian, Geronimo) whose journeys through Houston's Ben Taub reveal American healthcare's contradictions. Its difficulty for summarizers lies in its refusal of the polemical shortcut: Nuila is a practicing hospitalist and the son of a private-practice physician father whose politics oppose his own, so the book earns authority through lived tension rather than ideology.
The central thesis is deceptively simple and empirically grounded: a public hospital serving mostly uninsured patients delivers better outcomes at half the cost, proving that America's problem is not scarcity but structure. Nuila coins "Medicine Inc." to name the profit-driven amalgam of insurers, hospitals, and pharma whose foundational error is treating private insurance as the mandatory entry point to care. His most original clinical contribution is reframing lack of insurance as a diagnosable cause of disease, deserving a place on the differential alongside genetics and pathogens.
What elevates the book above policy tracts is its self-implication. Nuila confesses to "algorithmania" that killed time his dying grandmother needed, to burnout and suicidal ideation, to stereotyping his own Latino patients. This vulnerability inoculates the argument against preachiness. His policy prescription is notably moderate: not necessarily Medicare for All, which he doubts Americans want, but a universal floor with optional premium tiers, so that choice never determines survival.
The book's limitation is generalizability. Ben Taub benefits from local property-tax funding, teaching-hospital scale, and Houston's specific political compromise between a blue city and red state. Whether its model scales is unproven. Yet as a counterexample, it accomplishes something rare: it makes the impossible feel demonstrated. By naming "disaster syndrome," the resignation that accepts brokenness as permanent, Nuila diagnoses the reader's own passivity and insists, with Chekhov as his guide, that stories can be the hammer that awakens conscience.
People Also Read
Download PDF
Download EPUB
.epub digital book format is ideal for reading ebooks on phones, tablets, and e-readers.

































